Key points:
- The biologic refractory rheumatoid arthritis (RA) population accounts for approximately one-third of all RA patients who have received anti-TNF or other biologic agents, is the fastest growing branded market segment, the hardest to treat, and requires new therapies that are both effective and safe
- Intravenous infusions of allogeneic Mesenchymal Precursor Cells (MPCs) were well tolerated in biologic refractory RA patients and were without serious adverse events over 12 weeks
- A single intravenous MPC infusion in biologic refractory RA patients resulted in dose-related improvements in clinical symptoms, function, and disease activity, with the 2 million MPCs/kg dose providing the greatest benefit
- Importantly, ACR70, the most meaningful measure of clinical improvement, was achieved by significantly more of the high dose MPC-treated than placebo-treated patients at 12 weeks
- In patients who had previously received 1-2 biologics, a single infusion of 2 million MPC/kg resulted in 55% and 36% ACR50 and ACR70 responses, respectively, compared with 11% and 0% of placebo treated patients, and in 91% of patients achieving the minimum clinically important improvement in physical function, defined as a reduction of at least -0.22 in the HAQ-DI, compared with 33% placebo treated patients
- The safety and efficacy results of this trial provide support for the potential of Mesoblast’s allogeneic MPCs to be positioned as first-line treatment option in RA patients who have previously received a prior anti-TNF or other biologic agent
- Given the large market opportunity, Mesoblast’s Tier 1 product candidate, MPC-300-IV, is well-positioned to advance through a strategic partnership into Phase 3 development for biologic refractory rheumatoid arthritis
NEW YORK and MELBOURNE, Australia, Aug. 08, 2016 (GLOBE NEWSWIRE) — Mesoblast Limited (Nasdaq:MESO) (ASX:MSB) today announced that a single intravenous infusion of its proprietary allogeneic Mesenchymal Precursor Cell (MPC) product candidate, MPC-300-IV, was well tolerated and demonstrated a dose-related improvement in clinical symptoms, physical function, and disease activity relative to placebo through the 12 week primary endpoint in its Phase 2 trial in biologic refractory rheumatoid arthritis.
Dr Allan Gibofsky, Professor of Medicine and Public Health at Weill Cornell Medical College and Attending Rheumatologist at Hospital for Special Surgery in New York, commented: “The safety and efficacy results of this study are very encouraging and suggest that Mesoblast’s cell therapy has the potential to fill the major unmet medical need of the biologic refractory RA population, where agents that provide consistent durable effects without the risk of opportunistic infections or malignancies are sorely needed.”
Mesoblast’s Phase 2 trial recruited a total of 48 patients with active RA who were on a stable regimen of methotrexate and had an inadequate prior clinical response to at least one anti-Tumor Necrosis Factor (TNF) agent. Of the 48 patients, 30 (63%) had previously received 1-2 biologic agents. Patients were randomized to a single intravenous infusion of 1 million MPCs/kg (1M/kg, n=16), 2 million MPCs/kg (2M/kg, n=16) or placebo (n=16). The study was comprised of a 12 week primary study period with a 40 week follow-up for a study total duration of 52 weeks.
The primary objective of the study was to evaluate safety and tolerability of a single intravenous MPC infusion in these biologic refractory RA patients through a 12 week primary endpoint. Additional objectives were to evaluate clinical efficacy at the primary 12 week endpoint and to assess the durability of effects and safety profile through the full 52 week study. Pre-specified efficacy endpoints included the American College of Rheumatology (ACR) composite clinical response, which is an endpoint used in RA clinical trials to measure improvement in signs and symptoms of the disease in terms of 70%, 50% or 20% improvement from baseline, the health assessment questionnaire-disability index (HAQ-DI), a standardized measure of functional status, and the DAS28 composite measurement of disease activity. Analyses were performed for the whole study population and for the pre-specified exploratory subgroup based on whether the subjects had previously received 1-2 or more than 2 biologic agents.
Key results at week 12, shown in detail in the table below, were:
1. Safety:
- Cell infusions were well tolerated with no infusion-related adverse events. There were no serious adverse events, and the safety profile over 12 weeks was comparable among placebo and MPC treatment groups.
2. ACR70/50/20 composite scores measuring degree of clinical responses to treatment:
- There was a dose-related improvement in many of the individual components of the ACR composite following MPC treatment; the 2M/kg group who had previously received 1-2 biologics showed significant improvement over placebo in each of the following categories: swollen joint counts, investigator global assessment, patient global assessment, and patient pain scores.
- ACR70 responses overall showed a dose-related effect after a single MPC infusion, with the greatest effect seen in the 2M/kg group who had previously received 1-2 biologics (36% vs 0% placebo).
- ACR50 responses overall showed a dose-related effect after a single MPC infusion, with the greatest effect seen in the 2M/kg group who had previously received 1-2 biologics (55% vs 11% placebo).
- ACR20 responses were greater in both the 2M/kg and 1M/kg group who had previously received 1-2 biologics than placebo (55% and 60%, respectively, vs 33% placebo).
3. HAQ-DI score measuring functional improvement following treatment:
- A single MPC infusion resulted in a dose-related improvement in function, based on reduction in mean HAQ-DI levels as early as week 4 and sustained reduction in mean HAQ-DI through 12 weeks; maximal effect was seen in the 2M/kg group who had previously received 1-2 biologics (-0.7 vs -0.1 placebo).
- At 12 weeks, MPC treatment resulted in a dose-related increase in the number of patients achieving a minimum clinically important improvement in physical function, defined as a reduction of at least -0.22 in the HAQ-DI; the greatest effect was seen in the 2M/kg group who had previously received 1-2 biologics (91% vs 33% placebo).
4. DAS28 composite score measuring overall disease activity following treatment:
- A single MPC infusion resulted in a dose-related reduction in the mean DAS28 activity score relative to placebo, and in an increase in the number of patients achieving the biologically-meaningful target of low disease activity state, defined as DAS28-CRP <3.2.
Summary of Key Efficacy Responses at Week 12:
| All Subjects | Subgroup with Prior Use of 1-2 Biologics | |||||||||||||||||||
| Placebo | 1M/kg | 2M/kg | p-value 2M/kg vs placebo |
Placebo | 1M/kg | 2M/kg | p-value 2M/kg vs placebo |
|||||||||||||
| N=16 | N=16 | N=16 | N=9 | N=10 | N=11 | |||||||||||||||
| ACR70 | 0 | % | 20 | % | 27 | % | 0.04 | 0 | % | 20 | % | 36 | % | 0.09 | ||||||
| ACR50 | 19 | % | 27 | % | 31 | % | >0.1 | 11 | % | 30 | % | 55 | % | 0.07 | ||||||
| ACR20 | 50 | % | 47 | % | 50 | % | >0.1 | 33 | % | 60 | % | 55 | % | >0.1 | ||||||
| HAQ-DI <-0.22 | 38 | % | 53 | % | 93 | % | 0.003 | 33 | % | 60 | % | 91 | % | 0.02 | ||||||
| HAQ-DI LS mean change from baseline | -0.2 | -0.3 | -0.6 | 0.02 | -0.1 | -0.4 | -0.7 | 0.03 | ||||||||||||
| DAS28-CRP LS mean change from baseline | -1.4 | -1.3 | -2.0 | >0.1 | -1.1 | -1.8 | -2.4 | 0.06 | ||||||||||||
| DAS28-CRP <3.2 | 19 | % | 27 | % | 36 | % | >0.1 | 22 | % | 30 | % | 40 | % | >0.1 | ||||||
Major advances in the treatment of RA using biologic agents have resulted in a $15 billion global market in 2015, which is projected to grow to over $18 billion in 2024. Over two million patients were treated for RA in the United States alone in 2015, with three million more people in the five major European markets and Japan. Despite the substantial advances in RA treatment using biologic agents such as anti-TNF agents, approximately one third of patients either do not respond sufficiently or cannot tolerate these agents due to infectious or other complications. In the United States, the anti-TNF refractory population is the fastest growing branded market segment, projected to increase by 8% annually and potentially higher with the expected market entry and greater availability of anti-TNF biosimilars.
Mesoblast Chief Executive Silviu Itescu said: “The Phase 2 trial results have indicated a strong efficacy signal and consistent effects of a single MPC infusion on clinical symptoms, functional abilities, and disease activity, without any serious adverse events. These results support the potential of our allogeneic cell therapy to be positioned as a first-line treatment option for biologic refractory patients, where there is a clear need for safe and effective treatments. Given the large market opportunity, our Tier 1 product candidate, MPC-300-IV, is well-positioned to advance through a strategic partnership into Phase 3 development for biologic refractory rheumatoid arthritis.”
About Rheumatoid Arthritis
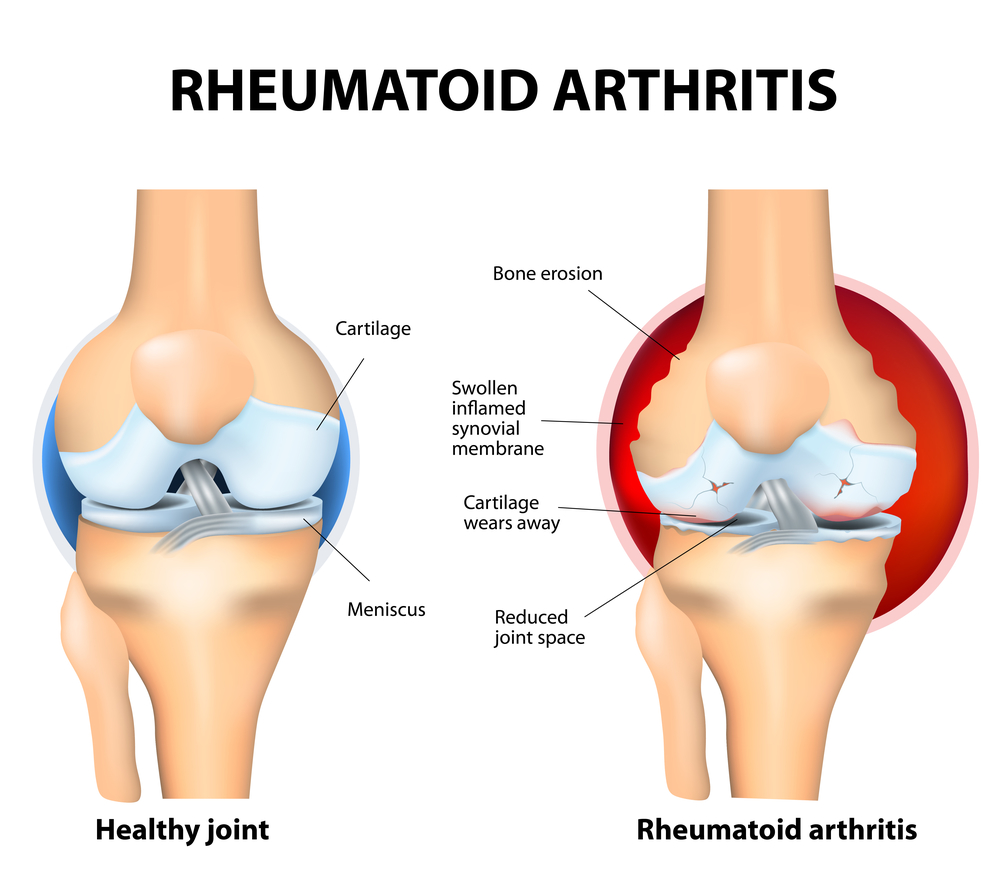
RA is a chronic autoimmune disease of unknown etiology, affecting approximately one percent of the global population. The disease is attributed to chronic inflammation affecting the synovial membrane of multiple joints, which eventually leads to cartilage and bone destruction. The health-related quality of life in patients with RA is significantly impaired by pain, fatigue, and decline in musculoskeletal function. RA is associated with an increased risk of cardiovascular disease and mortality.
Standard criteria established by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) are used to assess the effectiveness of RA treatments. The ACR70/50/20 response is a composite measure based on achieving 70%/50%/20% improvement in tender joint or swollen joint counts plus improvement in three of the following:
- Patient global assessment
- Physician global assessment
- Patient pain assessment
- Physical function/disability questionnaire (HAQ-DI)
- Acute phase reactant (sedimentation rate or high-sensitivity C-reactive protein)
The patient and physician global assessments and pain assessment are measured using a visual analogue scale on a scale of 0-100. The HAQ-DI assesses physical function in performing a variety of activities of daily living and yields a score ranging from 0-3 (lower is better). A reduction in the HAQ-DI score of -0.22 is the minimal clinically important difference.
The DAS28 is another validated RA disease activity index based on a 28 joint count. The derived DAS28 scores are comprised of tender joint count; swollen joint count; acute phase reactant (hsCRP or ESR) and the subject’s global assessment of disease but do not include measures of pain or physical function. High disease activity is defined as DAS28 score >5.1; moderate disease activity is defined as DAS28 scores between 5.1-3.2; low disease activity and remission are defined as DAS28 scores of <3.2 and <2.6, respectively.
About Mesoblast’s Product Candidate MPC-300-IV and Potential Mechanisms of Action
Mesoblast’s Tier 1 product candidate, MPC-300-IV, comprises 2 million immunoselected and culture-expanded Mesenchymal Precursor Cells (MPCs)/kilogram which are intravenously delivered. Existing biologic therapies target individual cytokine pathways thought to be involved in RA disease pathogenesis, including TNF-alpha, interleukin-6, or interleukin-17, but not concomitantly. There are at least two mechanisms of action (MOA) by which MPC-300-IV may impact on clinical rheumatoid arthritis outcomes through concomitant inhibition of multiple cytokine networks:
- Immunomodulatory MOA: Pro-inflammatory monocytes/macrophages and activated T cells are involved in the pathogenesis of RA via joint inflammation and secretion of multiple pro-inflammatory cytokines. In preclinical studies, activation of MPCs by these pro-inflammatory cytokines through specific surface receptors results in release by MPCs of anti-inflammatory mediators including PGE2 and IDO which act on inflammatory target cells. Allogeneic human MPCs secreting PGE2 and IDO, when co-cultured with donor immune cells, switch pro-inflammatory monocytes producing TNF-alpha or IL-6 to an anti-inflammatory phenotype producing IL-10, and switch pro-inflammatory T cells producing IL-17 to anti-inflammatory FoxP3 Tregs producing IL-10.
- Synoviocyte Inhibitory MOA: Pro-inflammatory synoviocytes in the RA joint proliferate highly and secrete multiple cytokines involved in RA disease pathogenesis. The biomolecules PGE2 and TGF-beta, secreted by MPCs following cell surface signalling by inflammatory cytokines, act directly on RA synoviocytes to inhibit the pleiotropic signalling molecule NFkappaB, resulting in reduced synoviocyte proliferation and decreased production by the synoviocytes of the pro-inflammatory factors TNF-alpha, IL-1, IL-6, IL-8, MCP-1, and various metalloproteinases involved in joint inflammation and destructive pathology.
In large animal studies, a single intravenous infusion of Mesoblast’s allogeneic MPCs resulted in concomitant inhibition of TNF-alpha, IL-6 and IL-17 inflammatory pathways in the inflamed joints, and substantially ameliorated clinical disease. Biologic refractory RA patients who have received prior anti-TNF or other biologic agents continue to have active inflammatory pathways, and the broad, concomitant targeting of multiple cytokine networks by MPCs may result in clinically meaningful outcomes in this patient group.
About Mesoblast
Mesoblast Limited (ASX:MSB; Nasdaq:MESO) is a global leader in developing innovative cell-based medicines. The Company has leveraged its proprietary technology platform, which is based on specialized cells known as mesenchymal lineage adult stem cells, to establish a broad portfolio of late-stage product candidates. Mesoblast’s allogeneic, ‘off-the-shelf’ cell product candidates target advanced stages of diseases with high, unmet medical needs including cardiovascular conditions, orthopedic disorders, immunologic and inflammatory disorders and oncologic/hematologic conditions.
Forward-Looking Statements
This press release includes forward-looking statements that relate to future events or our future financial performance and involve known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance or achievements to differ materially from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements. We make such forward-looking statements pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 and other federal securities laws. Forward-looking statements should not be read as a guarantee of future performance or results, and actual results may differ from the results anticipated in these forward-looking statements, and the differences may be material and adverse. You should read this press release together with our risk factors, in our most recently filed reports with the SEC or on our website. Uncertainties and risks that may cause Mesoblast’s actual results, performance or achievements to be materially different from those which may be expressed or implied by such statements, and accordingly, you should not place undue reliance on these forward-looking statements. We do not undertake any obligations to publicly update or revise any forward-looking statements, whether as a result of new information, future developments or otherwise.
For further information, please contact:
Schond Greenway
Investor Relations, Mesoblast
T: +1 212 880 2060
E: schond.greenway@mesoblast.com
Julie Meldrum
Corporate Communications, Mesoblast
T: +61 3 9639 6036
E: julie.meldrum@mesoblast.com